Meng Yu ![]() ,
Dao-Pei Zhang,
Ya-Fang Ren,
Hong-Tao Zhang,
Sheng-Qi Fu,
Shu-Ling Zhang
,
Dao-Pei Zhang,
Ya-Fang Ren,
Hong-Tao Zhang,
Sheng-Qi Fu,
Shu-Ling Zhang
For correspondence:- Meng Yu Email: ymyytjpr@163.com
Received: 12 April 2016 Accepted: 24 August 2016 Published: 30 September 2016
Citation: Yu M, Zhang D, Ren Y, Zhang H, Fu S, Zhang S. Clinical efficacy and safety of edaravone therapy in acute cerebral haemorrhage. Trop J Pharm Res 2016; 15(9):2029-2033 doi: 10.4314/tjpr.v15i9.30
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To evaluate the clinical efficacy and safety of edaravone in the treatment of acute cerebral haemorrhage (ACH).
Methods: This study recruited 120 patients who developed ACH. The patients were divided into control and treatment groups with 60 patients per group. The control group underwent conventional treatment and the treatment group also received intravenous edaravone. The volumes of cerebral edema and cerebral hematoma, high-sensitivity C-reactive protein (hs-CRP) and interleukin-6 (IL-6) levels, and Chinese Stroke Scale (CSS) score before and after treatment were compared between the two groups.
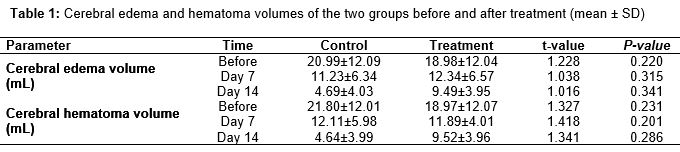
Results: The respective cerebral edema volumes of the control and treatment groups decreased from 20.99 ± 12.09 and 21.80 ± 12.01 mL on day 0 to 11.23 ± 6.34 and 12.11 ± 5.98 mL at day 7 and 4.69 ± 4.03 and 4.64 ± 3.9 mL on day 14 (P < 0.05). The respective cerebral hematoma volumes of the control and treatment groups decreased from 18.98 ± 12.04 and 18.97 ± 12.07 mL on day 0 to 12.34 ± 6.57 and 11.89 ± 4.01 mL at day 7 and 9.49 ± 3.95 and 9.52 ± 3.96 mL on day 14. Compared with pre-treatment, hs-CRP and IL-6 levels and CSS score of the two groups decreased significantly following treatment (p < 0.05); the differences in the cerebral edema and hematoma volumes of the two groups on days 7 and 14 were not significant (p > 0.05). The hs-CRP and IL-6 levels and CSS scores of the treatment group decreased appreciably (p < 0.05), while the incidence of adverse reactions in the treatment and control groups was 16.67 and 13.33 %, respectively, but the difference was not significant (p > 0.05).
Conclusion: Edaravone shows remarkable clinical efficacy and safety with no obvious adverse reactions in the treatment of ACH. Therefore, its use is recommended.
Introduction
Cerebral haemorrhage (CH) or encephalorrhagia is a form of “stroke” and is a common serious brain complication occurring in elderly patients with hypertension [1,2]. CH [3,4] refers to haemorrhage caused by the rupture of blood vessels in the non-traumatised brain parenchyma, and its most common causes include hypertension, cerebral arteriosclerosis, and intracranial vascular malformations. Because it is usually induced by force, agitation, and other factors, most cases occur during activity. CH, which usually happens suddenly [5], manifests as altered consciousness, limb paralysis, aphasia, and other neurological forms of damage. Characterised by its rapid incidence, critical condition, and high mortality rate, it can seriously affect patient health. Oxygen free radicals (OFRs) play an important role in cerebral edema and secondary cerebral injury. The compressive and stimulatory effect of a hematoma on brain tissues caused by acute cerebral haemorrhage (ACH) increase the production of OFRs, which aggravates cerebral ischemia and hypoxia [6,7].
Edaravone [8] is a new free radical scavenger with good lipophilicity that has 60 % permeability across the blood-brain barrier. It can scavenge free radicals, reduce the oxidative damage caused by polyunsaturated fatty acids, which are components of the cell phospholipid membrane, and inhibit neuronal apoptosis and cell peroxidation after a haemorrhage, relieving cerebral edema and cerebral tissue impairment.
Currently, edaravone is widely used in the early treatment of patients with acute cerebral infarction and its remarkable neuroprotective effect has been recognised [9]. Consequently, this study examined its use for the treatment of patients with ACH and compared its efficacy and safety with those of conventional treatment.
Methods
Study setting and design
This study enrolled 120 cases of ACH treated at Zhengzhou People’s Hospital from February, 2013 to December, 2014. All of the cases of ACH were confirmed using computed tomography (CT) or magnetic resonance imaging (MRI). Patients with systemic disease, haemorrhagic cerebral infarction, cerebral hernia, deep coma, severe complications, dementia, or severe mental disorders were excluded. All of the eligible patients gave informed consent and the study was approved by the medical ethics committee of Zhengzhou People’s Hospital (approval no: ZPH20150408YM) and followed the tenets of the Declaration of Helsinki [10]. The patients were divided into control and treatment groups using a random digital table method, with 60 per group. In the control group (mean age of 65.40 ± 2.40 (range 56 – 76) years; 34 men, 26 women); the average time from onset of CH to treatment was 0. 90 ± 1.40 (range 3 – 36) h; the bleeding site was the basal ganglia region in 20 cases, lobes in 22 cases, and thalamus in 18 cases (the largest oval grey matter nuclei in the diencephalon, distributed on both sides of the third cerebral ventricle); and the bleeding volume averaged 30.20 ± 2.90 (range 16 – 45) mL. In the treatment group (mean age 63.90 ± 2.60 (range 55 – 75) years; 32 men, 28 women) the average time from onset of CH to treatment was 23.50 ± 1.60 (range 4 – 39) h; the bleeding site was the basal ganglia region in 18 cases, lobes in 26 cases, and thalamus in 16 cases; and the average bleeding volume was 32.10 ± 2.50 (range 17 – 48 mL) mL. The two patient groups did not differ statistically (p < 0.05); therefore, the results of the two groups were comparable.
Treatment
Patients in the control group were given symptomatic and supportive treatment such as blood pressure control, intracranial pressure reduction, blood pressure adjustment and infection prevention. In addition, the patients in the treatment group were treated with intravenous edaravone 30 mg in 100 mL of normal saline, twice per day. Two weeks was considered one course of treatment.
Observation index
The cerebral edema and hematoma volumes, the levels of high-sensitivity C-reactive protein (hs-CRP) and interleukin-6 (IL-6), and Chinese stroke scale (CSS) score were compared at days 7 and 14. The cerebral edema and hematoma volumes were measured using hematoma volume measurement software. The hs-CRP and IL-6 levels were determined in fasting venous blood samples using immunoturbidimetry and a radioimmunoassay, respectively, as per the kit instructions.
Statistical analysis
SPSS 19.0 was used for data processing. Numeric data were compared using Chi-square test. Data are expressed as mean ± standard deviation (SD) and t-test was used to analyse differences between group data. Differences were considered statistically significant if p < 0.05.
Results
Changes in cerebral edema and hematoma volumes
Before treatment, the differences in the cerebral edema and hematoma volumes between the two groups were not significant (p > 0.05); the cerebral edema and hematoma volumes decreased significantly in both groups 7 and 14 days after treatment, although the differences between the control and treatment groups were not significant (p > 0.05) ().
hs-CRP and IL-6 levels, and CSS score
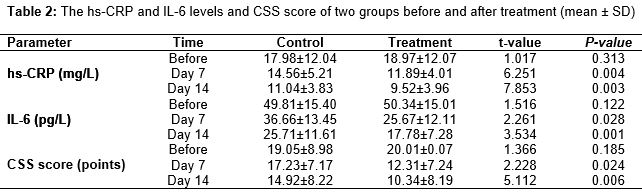
On days 7 and 14 after treatment, the hs-CRP and IL-6 levels and CSS score were decreased compared with day 0 for both groups (p > 0.05), and the reduction in the indices was more remarkable in the treatment group than in the controls (p < 0.05) ().
Adverse reactions
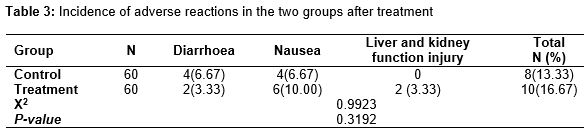
The incidence of adverse reactions in the control group was 13.33 % and included four cases of diarrhoea, four cases of nausea, and no case of liver or kidney function injury; for the treatment group, the incidence of adverse reactions was 16.67 %, including two cases of diarrhoea, six cases of nausea, and two cases of liver and kidney function injury; the difference in the incidence of adverse reactions between the two groups was not significant (p > 0.05) ().
Discussion
Cerebral haemorrhage is an acute cerebrovascular disease with a high incidence that has a high disability rate and mortality. The increased intracranial pressure after ACH causes ischemic injury in the brain tissue around the haematoma [11], which accelerates the metabolism of arachidonic acid in brain tissue and induces an increase in free radicals. A severe inflammatory reaction occurs in the damaged area, which induces the generation of large amounts of oxygen radicals and superoxide anion free radicals. The major pathological mechanism of the free radical injury is the induction of lipid peroxidation [12,13]. The brain is very sensitive to OFRs because brain tissue contains abundant lipids. A large number of OFRs can damage the lysosomal membrane of brain cells, and various hydrolytic enzymes that are released into the cytoplasm can further injure the nerve cells. The red blood cells in the hematoma release a large amount of haemoglobin after being damaged.
Currently, much attention in the treatment of ACH has focused on the important role of free radicals in the mechanism of ACH [14]. The free radical scavenger edaravone is widely used in the treatment of acute cerebral infarction; it inhibits the lipid peroxidation process and affects the expression of apoptosis-related genes by scavenging OFRs in body tissues, thereby reducing the further damage caused by active oxygen and promoting the recovery of neurological function. One study [15] reported that administering edaravone in the treatment of ACH had remarkable clinical effect, without affecting blood coagulation, the platelet aggregation process, or bleeding time. Chen et al. [16] found that treating patients with acute cerebral ischemic stroke with edaravone limited the reduction in local cerebral blood flow around the infarcted region. A rat study [17] demonstrated that the intravenous injection of edaravone in animals undergoing ischemia reperfusion blocked the progress of cerebral edema and cerebral infarction, relieved neural symptoms, and limited delayed neuron death. In our study, the cerebral edema and hematoma volumes were significantly smaller in the control and treatment groups after treatment than before treatment, and the curative effect was better in the treatment group. The difference in the incidence of untoward reactions in the two groups was not significant (p > 0.05), which was consistent with the research results mentioned above.
Hs-CPR and IL-6 are both important markers of inflammatory reaction. Edaravone markedly suppresses inflammatory markers and inflammatory factors, including hs-CPR and IL-6, reducing further damage following ACH [18]. In our study, the hs-CRP and IL-6 levels of the two groups decreased dramatically after treatment (p < 0.05), but the reduction was more remarkable in the treatment group (p < 0.05). This indicates that treating ACH using edaravone in combination with conventional therapy can significantly reduce hs-CRP and IL-6 levels.
Limitations of the study
No significant difference was observed in the reduction in the volumes of cerebral edema and cerebral hematoma between the two groups, which is inconsistent with previous studies. This may be due to the small sample size used. Studies with a large sample size need to be conducted.
Conclusion
The findings of this study indicate that edaravone combined with conventional therapy is beneficial to the recovery of nerve function and improvement in daily activities when used in the treatment of ACH. During the treatment period, no obvious adverse effects and aggravated disease conditions were seen, which further implies that edaravone is safe and effective in the treatment of ACH.
Declarations
Acknowledgement
References
Archives


News Updates